

INTRODUCTION
Percutaneous coronary intervention (PCI) is an effective method of coronar y revascularization to identify the presence and extent of atherosclerotic coronary artery disease (CAD). There are specific complications that are dependent on the patients and are related to the procedure, especially fever, which indicate infection due to invasive procedures such as coronary angiography or PCI [1]. The incidence of fever complicating PCI is rare, and the reported rate of infection in patients undergoing PCI is less than 1% [2,3]. However, mild fever is a common phenomenon in patients with acute myocardial infarction (AMI) and has been recognized as a nonspecific response to myocardial damage. Body temperature (BT) can increase by an average of 1℃ or more as early as 4-8 hours from onset of infarction, and it usually resolves after 4-5 days [4]. Development of fever in patients with AMI is associated with elevated serum levels of myocardial enzymes and high-sensitivity C-reactive protein (hsCRP) [5,6]. Fever after AMI is an independent predictor of adverse clinical outcomes. However, its causality and pathological mechanisms remain poorly understood [7]. Other subsequent studies have demonstrated that fever after AMI is a predictor of infarct size and left ventricular remodeling [8,9]. In addition, cardiogenic shock complicating AMI is often accompanied by a systemic inflammatory response, and is associated with multiorgan failure and high mortality rates. The extent of the overlap between cardiogenic shock and other conditions that lead to a systemic inflammatory state is unclear [10-12]. However, little is known about the cause of fever after PCI in patients with AMI.
Therefore, this study aimed to determine the long-term clinical outcomes and clinical characteristics of patients with AMI who developed fever after PCI, and to investigate the factors that may affect the development of fever.
METHODS
1. Study design and population
We studied patients who developed after undergoing PCI for AMI between March 2010 and December 2019 at Jeju National University Hospital in Korea. AMI included ST-segment elevation MI (STEMI) and non-STEMI (NSTEMI). The inclusion criteria for the present analysis were as follows: patients aged ≥18 years, patients demonstrating STEMI or NSTEMI, and patients undergoing PCI. The investigators defined AMI as per the universal definition of MI [13].
This study was approved by the Institutional Review Board (IRB) of Jeju National University Hospital (IRB No. 2022-02-001). The requirement for informed consent was waived by the IRB.
2. Study definitions, PCI procedures and medical treatment
STEMI was defined as the experience of chest pain with ST-segment elevation ≥2 mm in ≥2 contiguous precordial leads, ≥1 mm in ≥2 limb leads, or new-onset left bundle branch block on electrocardiogram at admission, along with elevation of cardiac enzymes to at least more than three times the upper limit of the normal range [14]. If the patients showed an absence of persistent ST-segment elevation, with increased cardiac biomarkers, and the clinical context was appropriate, the patients were considered to have NSTEMI [15,16]. Diagnostic coronary angiography and PCI were performed through either the femoral or the radial artery after administration of unfractionated hepar in (50 to 100 I U/ kg), according to the general standard PCI guidelines [17]. Before PCI, all the patients were administered loading doses of 200-300 mg of aspirin and other antiplatelet agents. Coronary revascularization was defined as ≥70% diameter restenosis in a coronary artery by visual estimation, or the occurrence of typical angina and/or presentation of signs of ischemia and ≥50% diameter restenosis. During the in-hospital period, the patients received antiplatelet agents, beta-blockers, renin-angiotensin-aldosterone system inhibitors, calcium channel blockers, and lipid-lowering agents. After discharge, patients were encouraged to stay on the same medications that they received during hospitalization. The total duration of the dual antiplatelet therapy was recommended to be more than 12 months in patients who had undergone PCI. The left ventricular (LV) wall motion score index (WMSI) was assessed using a 16-segment model [18]. Segmental wall motion was assessed by an experienced cardiologist as normal=1, hypokinetic=2, akinetic=3, and dyskinetic=4. Clinical follow-ups were routinely performed by visiting the outpatient department of cardiology at 6, 12, and 24 months, and whenever any clinical events occurred. If patients did not visit the hospital, outcome data were assessed via telephone interviews. The clinical events were not centrally adjudicated. The physician identified all the events, and the principal investigator of each hospital confirmed the events.
The exclusion criteria were as follows: fever before admission, active inf lammatory or infectious diseases, recent antibiotic consumption, use of thrombolytic agents, development of infarct-related mechanical complications, current treatment with corticosteroids, coronary artery bypass grafting, and therapeutic hypothermia. The duration of PCI was defined as the time from arrival to departure from the angiography room.
BT was measured every 4 or 8 hours during hospitalization using an infrared ear thermometer. Fever was defined as peak ear BT of more than 37.7℃. The patients were divided into two groups according to the presence or absence of fever after PCI. The fever group had BT ≥37.7℃, and the no-fever group had BT <37.7℃.
3. Culture study
If the BT of patients undergoing PCI was above 37.7℃, they underwent physical examination as well as imaging and culture study to exclude infections. Culture studies included two pairs of blood, urine, sputum, and wound cultures, if the patients had a wound. If a culture was obtained, the site of the culture, type of organism detected by the culture, and the outcome were recorded. We detected organisms on culture studies by reviewing the list of positive cultures processed by the clinical microbiology laboratory at Jeju National University Hospital.
4. Statistical analysis
For continuous variables, differences between the two groups were evaluated using Student’s t -test. Data were expressed as mean±standard deviation. For discrete variables, differences were expressed as counts and percentages and analyzed using the chi-square test. Various clinical outcomes up to 2 years were estimated using the Kaplan-Meier analysis, and differences between the groups were compared using the log-rank test. Univariate and multivariate Cox proportional hazard models were used to analyze prognostic factors for mortality at 2 years. Statistical analyses were performed using SPSS version 20.0 for Windows (IBM, Markham, Canada), and a P-value of less than 0.05 was considered statistically significant.
RESULTS
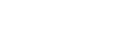
A total of 926 patients with AMI were enrolled in this study. We excluded 41 patients without PCI, 11 patients who developed fever before PCI, three patients with recent antibiotic consumption, two patients with corticosteroid treatment, and three patients with tracheal intubation before PCI. The remaining 866 patients were analyzed in this study. A total of 130 patients developed fever after PCI (fever group), while 736 patients did not (no-fever group) (Fig. 1).
1. Baseline clinical characteristics
Baseline characteristics of this study population are summarized in Table 1. The patients in the fever group were more likely to be female, had a higher prevalence of chronic kidney disease (CKD), and a longer duration of PCI. Systolic blood pressure, diastolic blood pressure, BT at admission, and LV ejection fraction (LVEF) after PCI in the fever group were lower than those in the non-fever group. In laboratory findings, white blood cell (WBC) count, hsCRP level, and peak creatine kinase-myocardial band (CKMB) were higher in the fever group, and other laborator y findings were not different between the groups. The rates of AMI and multivessel disease did not differ between the two groups.
2. Clinical outcomes
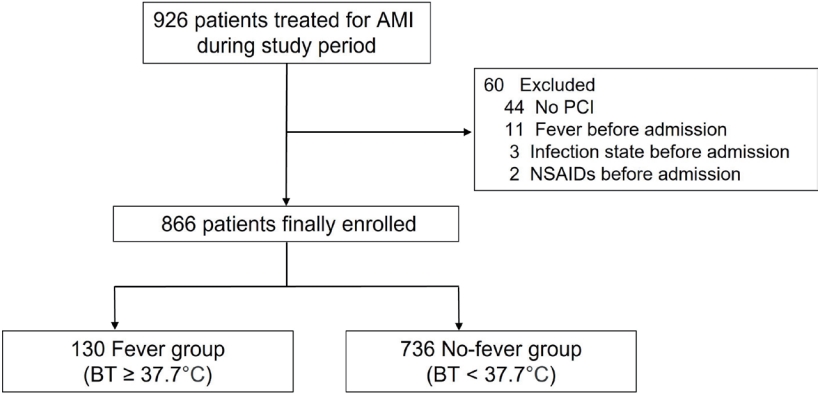
Various clinical outcomes of the 2 years follow-up were analyzed using Cox proportional hazards ratio model analysis and Kaplan-Meier curve analysis, as shown in Fig. 2 and Table 2. Fever after PCI was associated with higher incidence of major adverse cardiac events (MACE) (hazard ratio [HR], 1.56; 95% confidence interval [CI], 1.07-2.28; P=0.021) (Fig. 2A), all-cause death (HR, 2.32; 95% CI, 1.18-4.45; P=0.014) (Fig. 2B), cardiac death (CD) (HR, 2.57; 95% CI, 1.02-6.76; P=0.049) (Fig. 2C) and any revascularization (HR, 1.69; 95% CI, 1.02-2.81; P=0.044) (Fig. 2D) than without fever. However, there was no significant difference in the incidence of recurrent MI, CVA, re-hospitalization due to heart failure, or stent thrombosis between the two groups.
Subgroup analyses were performed to compare the clinical outcomes according to LVEF (Table 3, Fig. 3). In patients with decreased LVEF (<50%), the incidence of MACE, re-hospitalization due to HF, and stent thrombosis was higher than that in patients with preserved LVEF (≥50%). The incidence of other clinical outcomes did not differ significantly between the groups. In patients with decreased LVEF, fever after PCI was associated with a higher incidence of any revascularization (HR, 2.11; 95% CI, 1.02-4.35; P =0.043); however, there was no significant difference in the incidence of other clinical outcomes. In patients with preserved LVEF, fever after PCI was not associated with the 2 years clinical outcomes.
3. Predictors of developing fever after PCI
Regression analysis was performed to evaluate predictors of fever after PCI (Table 4). In women, prior CKD, lower LVEF, higher LV WMSI, WBC count, peak CKMB level, and longer PCI duration were associated with fever after PCI. Procedures such as intra-aortic balloon pump (IABP), extracorporeal membrane oxygenation (ECMO), continuous renal replacement therapy (CRRT), central line insertion, arterial line insertion, and cardiopulmonary resuscitation (CPR) were associated with fever after PCI. However, hsCRP or the procedural approach were not associated with the development the development of fever after PCI.
4. Culture study
Culture studies were performed on the patients in the fever group. Culture results were positive in 30 patients (23.1% of the ten groups). Positive culture was found in 11 cases in blood culture, 13 cases in sputum, and 11 cases in urine. The main organisms of infection were coagulase-negative Staphylococcus, Escherichia coli, Klebsiella pneumoniae, and Staphylococcus aureus (Table 5).
DISCUSSION
The main findings of this study showed that fever after PCI was associated with a higher incidence of MACE, all-cause death, CD, and any revascularization in patients with AMI who survived the initial attack up to 2 years of follow-up. Fever after PCI was not associated with recurrent MI, CVA, rehospitalization, or stent thrombosis. The subgroup analysis revealed that decreased LVEF was associated with a higher incidence of MACE, re-hospitalization due to HF, and stent thrombosis. Predictors of development of fever after PCI were female sex, prior CKD, LVEF, LV WMSI, WBC count, peak CKMB level, duration of PCI, and procedures in the angiography room such as IABP, ECMP, CRRT, central line insertion, arterial line insertion, intubation, and CPR. Most patients with fever after PCI had negative culture studies. In cases of positive results (23.1% of the fever group), the main pathogen was coagulase-negative Staphylococcus.
Fever in AMI was previously recognized as a nonspecific inflammatory response due to myocardial tissue necrosis. However, in many subsequent reports, fever after AMI was associated with another underlying mechanism. Fever after PCI may impair cardiovascular function by increasing myocardial oxygen requirements, possibly predisposing to the extension of the myocardial infarct and arrhythmias [8]. In a clinical study, the peak 24 hour BT after AMI in the ear of primary PCI was related to the infarct size, but not to a nonspecific inf lammatory response [9]. In another study, increased BT after AMI may have been associated with the expansion of the myocardial infarct, suggesting a relationship between systemic inf lammatory response and LV remodeling [19]. Therefore, fever after AMI can be understood not only as a secondary phenomenon according to myocardial necrosis, but also as a predictor of infarct size.
In this study, WBC count and hsCRP level were higher in the fever group than in the no-fever group. Elevated WBC counts and hsCRP levels represented more active inf lammation in the fever group. By producing tissue factors, for mi ng platelet-leu kocy te agg regates, and providing a catalytic surface for thrombin generation, leukocytes may exert a prothrombotic effect [20-22]. In a recent clinical trial, the WBC count at admission with STEMI was an independent predictor of infarct size as well as the 1 year mortality after PCI [23]. The hsCRP, which is an acute-phase reactant, plays an important role in the immune response, and is recognized as a mediator of atherosclerosis [24]. Elevated serum hsCRP levels predict worse short- and long-term prognosis in AMI as well as recurrent in-hospital cardiac events [25-27]. Therefore, more active inf lammation in the fever group might be the reason for higher all-cause mortality.
A previous study evaluated infarct size in patients with AMI after PCI using biomarker levels and echocardiography [9]. There was a statistically significant correlation between the 24 hours peak BT and the CKMB level, troponin level, and LV WMSI, indicating that fever after AMI is correlated with the degree of myocardial necrosis. Peak CK-MB level was the best predictor of LV WMSI, and BT was correlated with LV WMSI. In this study, peak CK-MB levels were also associated with fever after PCI in patients with AMI.
In a previous study, a longer PCI duration was associated with fever after PCI, and a more positive culture study was found [28]. Also, in this study, a longer PCI duration was a predictor of fever after PCI, suggesting that IABP, ECMO, CRRT, central line insertion, arterial line insertion, intubation, and CPR treatment during PCI may have affected the PCI duration.
S. aureus is the main cause of nosocomial infection, and S. aureus infection is a very rare but serious complication that is associated with mortality and length of hospitalization [29]. Bacterial growth in blood cultures after cardiac catheterization may be due to many possible scenarios, such as contamination during the procedure, contamination during specimen processing, transient bacteremia that resolves spontaneously, true bloodstream infection unrelated to the procedure itself, and true bloodstream infection caused directly by the invasive procedure itself. In this study, unlike previous studies, 23.1% of the fever group was positive for the culture studies, and various organisms were found, suggesting that the culture test was positive due to various causes.
This study had several limitations. First, this was a retrospective and a single-center study. This may have introduced a selection bias. Second, although various examinations such as chest radiography, blood culture, urine analysis, and sputum culture were performed to exclude the possibility of systemic infection, there could be an undetermined infection. Third, we measured BT using an infrared ear thermometer on admission, and even if the BT is above 37.7℃, it may be different from the central BT. Finally, detailed pyrogenic factors, such as interleukin or complement, were not assessed.
In conclusion, fever after PCI in AMI patients who survived the initial attack was associated with a higher incidence of MACE, all-cause death, CD, and any revascularization up to 2 years of follow-up than in those without fever after PCI.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






